57M Tb cervical lymphadenopathy pancytopenia on ATT
This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's consent. Here we discuss our individual patient's problems through a series of inputs from the available global online community of experts with the aim to solve those patients' clinical problems with the collective current best evidence-based input.
Case History
9 months ago, a small "gadda" appeared on the neck. FNAC was performed, and the report at that time were same as the current report. Sputum test was negative. Based on the analysis of the "gadda," TB symptoms were suspected. Medications were started and continued for 5 months., during which the "gadda" began improving. For the first month of treatment, everything was fine, but fever episodes started appearing after that. These fevers occurred twice a month, lasting about 5-10 days each time.
In October, the patient experienced low platelet counts and a jaundice episode. After a month of treatment, the platelets improved. When the fever occurred again in November, they took the patient to pulmonologist. Tests were done and same TB medications continued. On the 1st week of November, platelets dropped again and they took the patient to a hospital in Hyderabad where the treatment is ongoing.
His urine report is normal but his HB levels are decreasing.
Fever Details:
Whenever the fever occurs, it lasts for 5–10 days, and no treatment seems effective during that period. It resolves on its own. The fever reaches 102°/103°, and recovery from the symptoms and fever episodes takes about 15 days. There is always a shivering followed by the fever. Whenever the patient started to shiver, the family understood that he will have a fever now. Ten days before the fever, "gadda" starts to get "mota". As the fever reduces, "gadda" reduces. Before the TB treatment, the "gadda" remained consistently "mota", but with medications it now stays normal, except before fever episodes.
Background:
The patient has diabetes for 3-4 years and it remains on border. Medications for diabetes started and is continued till this date managed with 1 tablet daily. There is no history of hypertension or other physical issues.
He was a car driver by occupation. He smoked 4-5 cigarettes daily and drank alcohol for 30 years, both of which he stopped entirely after the TB diagnosis. Now he rests at home. His appetite is good, which only decreases during fever episodes. His mood remains normal, as it was before.


PaJR PHR Moderator: Thanks. Please also help him to insert the other components of soap here @Participant.
Participant:
S: C/o FEVER -
O:
On examination
Patient is conscious coherent and cooperative. No Pallor, Icterus, cyanosis, clubbing, edema.
Cervical lymphadenopathy +
Vitals:
Temp: 99.2 (10:00 am)
PR:84 BPM
BP:110/70 MM/HG
GRBS: 172 mg/dl(10:00 am)
7 points GRBS:
28/11
10AM : 167mg/dl
2PM : 129 mg/dl
8PM: 105mg/dl
10 PM: 210 mg/dl
29/11
2AM: 117mg/dl
8 Am : 114 mg/dl
CVS: S1 ,S2 heard
RS:B/L AE present,nvbs
P/A:Soft, non tender
No rigidity,Guarding.
CNS:NAD
A:Pancytopenia 2* to ? ATT ?Bone marrow suppression
K/c/o TB cervical lymphadenitis
P
1.IV FLUIDS 1 • Ns @ 50 ml/hr
2.Inj NEOMOL- 1 g iv/sos
3.TAB pcm 650mg po/qid
4.TAB. BENADON 40 mg PO/OD
5.TAB. METFORMIN 500mg PO/OD
6.TAB. MVT po/od 2pm
7.PAN 40mg po/od
PaJR PHR Moderator: Subjectively complains of fever when? Can't have complained of it at 4PM on 28th!
Participant: Sir pt subjectively complains of only one fever spike in 24 hrs
PaJR PHR Moderator: Rest of the time how is he subjectively?
30/11/24

PaJR PHR Moderator: Please mention the daily subjectivities recorded in the daily notes and include the daily investigations in the objectivities below the fever data
Participant: Okay sir

02/12/24
Participant:






PaJR PHR Moderator: 👍 let's also have the chart today @Participant
Participant:

PaJR PHR Moderator: Please share the fever chart
Participant:

PaJR PHR Moderator:

PaJR PHR Moderator: Today's fever chart update?
05/12/24
PaJR PHR Moderator: Today's fever chart update? @Participant
Lymph node biopsy update?
Participant: Patient got discharged sir
They will come after one week sir
PaJR PHR Moderator: Can we have the last picture of the fever chart?
09/12/24

PaJR PHR Moderator: Let's plan for his cervical lymph nodes biopsy but meanwhile how is his fever and how is he subjectively @Narmeen Shah @Patient Advocate ?

Participant: No fever and he is subjectively good sir
PaJR PHR Moderator: Reviewing him again in OPD @Narmeen Shah
Participant: Brig sir told to repeat fnac
And take oncosurgeon opinion and get Ct done as the lymph node is close to carotid and then he will do biopsy sir
PaJR PHR Moderator: Alright let's repeat the FNAC and get him shown to the onco surg this Wednesday
Did you PM me his IP number so that we can add his EMR summary to @Narmeen Shah 's case report?
PaJR PHR Moderator: @Narmeen Shah fresh clinical images to upload
where this bulge near the angle of the mandible is a large palpable lymph node

PaJR PHR Moderator: EMR Summary
Age/Gender : 57 Years/Male
Address :
Discharge Type: Relieved
Admission Date: 25/11/2024 01:05 PM
Diagnosis
PANCYTOPENIA SECONDARY TO ? BONE MARROW SUPPRESSION SECONDARY TO ? RIFAMPACIN INDUCED ?SINUS HISTOCYTOSIS WITH MASSIVE LYMPHADENOPATHY
?HODGKINS LYMPHOMA
K/C/O TB,CERVICAL LYMPHADENOPATHY K/C/O T2 DM SINCE 3 MONTHS
Case History and Clinical Findings
Chief COMPLAINTS :
C/O FEVER SINCE 5 DAYS
HISTORY OF PRESENTING ILLNESS:
PATIENT WAS Apparently SYMPTOMATIC 5 DAYS AGO AND THEN HE DEVELOPED FEVER SINCE 5 DAYS, AND THEN HIGH GRADE, CHILLS AND RIGIDITY Continuous TYPE ,NO COLD AND COUGH
H/O FEVER WITH THROMBOCYTOPENIA ADMISSION 2 TIMES
NO H/O COLD COUGH ALLERGIES CHESTPAIN, PALPITATION, SWEATING,SOB,ABD PAIN, NAUSEA, VOMITING,LOOSE STOOLS,BURNING MICTURATION,CONSTIPATION
PAST HISTORY:
K/C/O DM T2 SINCE 4 YEARS AND ON TAB METFORMIN 500MG PO/OD H/O PTB SINCE 4 MONTHS AND ON ATT DRUGS
N/K/C/O HTN, EPILEPSY, ASTHAMA, CVA,CVD GENERAL EXAMINATION :
PATIENT IS C/C/C NO PALLOR, ICTERUS, CYANOSIS, CLUBBING, LYMPHEDENOPATHY, EDEMA
BP : 100/70 PR:78BPM RR: 21CPM
SPO2: 98%@RA TEMP: 101.2
SYSTEMIC EXAMINATION :
CVS S1S2 + CNS NFND RS BAE + P/A SOFT,NT
PULMO REFRAL DONE ON26/11/2024 I/V/O CONSEDERATION SECOND LINE ATT AND FEVER SPIKES
ADV HOLD ATT
USG DONE ON 26/11/2024
IMPRESSION B/L RENAL CORTICAL CYST,MILD SPLEENOMEGALY, GB WALL EDEMA USG OF NECK DONE ON 2/12/2024 I/V/O CERVICAL LYMPHNODE SWELLING IMPRESSION CERVICAL LYMPHADENOPATHY
SPONGY FORM NODLES IN THYROID
ATHEROSLEROTIC CHANGES IN RIGHT ICA AND CALCIFIED ATHEROSCLEROTIC PLAQUES IN LEFT ICA
BONE MARROW ASPIRATION AND BIOPSY DONE ON 30/11/2024 /V/O PANCYTOPENIA
Investigation
RFT UREA 32 mg/dl 42-12 mg/dlCREATININE 0.8 mg/dl 1.3-0.9 mg/dlURIC ACID 2.0 mmol/L 7.2-3.5
mmol/LCALCIUM 9.9 mg/dl 10.2-8.6 mg/dlPHOSPHOROUS 2.7 mg/dl 4.5-2.5 mg/dlSODIUM 129
mmol/L 145-136 mmol/LPOTASSIUM 4.3 mmol/L. 5.1-3.5 mmol/L.CHLORIDE 96 mmol/L 98-107 mmol/L
LIVER FUNCTION TEST (LFT) Total Bilurubin 1.18 mg/dl 1-0 mg/dlDirect Bilurubin 0.20 mg/dl 0.2-
0.0 mg/dlSGOT(AST) 29 IU/L 35-0 IU/LSGPT(ALT) 13 IU/L 45-0 IU/LALKALINE PHOSPHATASE
445 IU/L 128-53 IU/LTOTAL PROTEINS 5.3 gm/dl 8.3-6.4 gm/dlALBUMIN 3.01 gm/dl 5.2-3.5
gm/dlA/G RATIO 1.31
COMPLETE URINE EXAMINATION (CUE) COLOUR Pale yellowAPPEARANCE ClearREACTION AcidicSP.GRAVITY 1.010ALBUMIN +SUGAR NilBILE SALTS NilBILE PIGMENTS NilPUS CELLS 2- 4EPITHELIAL CELLS 2-3RED BLOOD CELLS NilCRYSTALS NilCASTS NilAMORPHOUS
DEPOSITS Absent
OTHERS Nil
HBsAg-RAPID NegativeAnti HCV Antibodies - RAPID Non Reactive
SERUM ELECTROLYTES (Na, K, C l) SODIUM 128 mmol/L 145-136 mmol/LPOTASSIUM 4.2 mmol/L 5.1-3.5 mmol/LCHLORIDE 95 mmol/L 98-107 mmol/LPOST LUNCH BLOOD SUGAR 205
mg/dl 140-0 mg/dl HEMOGRAM 2/12/2024 HB 7.2
TC 3,700
N/L/E/M/B 47/35/02/16/00 RBC 2.36
PLT 1.20
COURSE IN THE HOSPITAL :
PT PRESENTED TO GM OPD WITH C/O FEVER SINCE 5 DAYS AND FURTHER EVALUTION PANCYTOPENIA IS PRESENT PT WAS DIAGNOSED AS TB LYMPHADENITIS AND STATED ON ATT IN SINCE JUNE, SINCE 6 MONTHS, PT HAD FEVER SPIKES ON AND OFF . SINCE 2 MONTHS PT HAD PANCYTOPENIA, PULMO OPINION WAS TAKEN I/V/O PANCYTOPENIA SECONDARY TO RIFAMPACIN AND ADVICED TO STOP ATT DRUGS AND CONTINOIUS FEVER SPIKES WAS PRESENT AND GIVEN ANTIPYRETICS . BONE MARROW ASPIRATION AND BIOPSY WAS DONE I/V/O PANCYTOPENIAAND REPORTS AWAITED. PT HAD NO FEVER SPIKES SINCE 2 DAYS AND HE IS HEMODINAMICALLY STABLE AT THE TIME OF DISCHARGE.
Treatment Given(Enter only Generic Name)
IVF NS @50ML/HR
TAB PCM 650MG PO/SOS
TAB METFORMIN 500 MG PO/BD TAB MVT PO/OD
TAB PAN 40MG PO/OD
Advice at Discharge
TAB PCM 650MG PO/SOS
TAB METFORMIN 500 MG PO/BD TAB MVT PO/OD
TAB PAN 40MG PO/OD
Follow Up
REVIEW TO GM OPD AFTER 1WEEK /SOS
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE, DONOT MISS MEDICATIONS. In case of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: ___________. For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER SIGNATURE OF PG/INTERNEE SIGNATURE OF ADMINISTRATOR SIGNATURE OF FACULTY
Discharge Date Date:4/12/2024 Ward: AMC Unit:I

PaJR PHR Moderator: Please share every 4 hours so that @Narmeen Shah can prepare the graph
Participant: Fnac was done yesterday on Op basis sir
PaJR PHR Moderator: Results tomorrow?
Participant: Yes sir
He has high grade fever since yesterday sir
PaJR PHR Moderator: We need to know the temperature readings four hourly
What is the temperature now @Patient Advocate
Patient Advocate:

16/12/24
Participant:



PaJR PHR Moderator: In view of the lymph-nodal organisms we may need to attribute this to a myelophthisic anemia.

PaJR PHR Moderator:



Participant:


PaJR PHR Moderator:
Participant: CBNAAT is negative
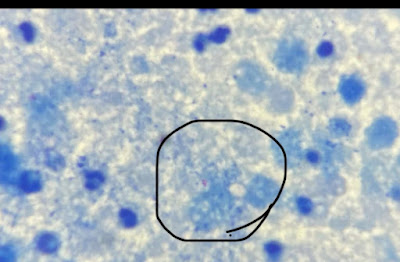
PaJR PHR Moderator: Then are those pink globi really AFB or even if they are they are likely NTM that won't be picked up on CBNAAT probes with fixed ontologies? We definitely need to culture this one after Microbiology today confirms these are AFB!
PaJR PHR Moderator: Feedback from our Microbiology professor on looking at the image:
[19/12, 08:42] Prof Microbology:
That is stain sir. Some pockets may not get decolourised completely during staining. That is why typical morphology we will look for.
This usually happen and one of the reasons for false positives.
[19/12, 08:50] : So it's possible that it's not even NTM?
[19/12, 09:10] PaJR PHR Moderator: Also those apparent AFBs? Could they be staining artifacts?
I'm sending our PG to gather the slides to show Prof Sai Leela in Microbiology. Where can they meet you to collect it and do they need another permission request letter to collect it?
[19/12, 09:10] Assoc Prof Pathology: Yes sir
[19/12, 09:10] Assoc Prof Pathology: But they are filled in macrophages only sir
[19/12, 09:11] Assoc Prof Pathology: Yes sir better if slide is reviewed by microbiologist
[19/12, 09:11] Assoc Prof Pathology: Pathology department sir
[19/12, 09:11] Assoc Prof Pathology: Letter should be sent sir and slides wll be given at cytopath section near lab
PaJR PHR Moderator: @Participant were you able to get the letter or the slides?
Participant: Collected slides and I am with sai Leela mam sir

PaJR PHR Moderator: OMG this slide looks loaded! Wonder what happened to that patient!
PaJR PHR Moderator:
[19/12, 13:17] Prof Microbology: Sir,
I have seen the slide sir
No acid fast bacilli seen
[19/12, 13:18] Prof Microbology: Bacilli were seen which are non acid fast
0/12/24
PaJR PHR Moderator:
[20/12, 07:37] PG: Sir
We r planning to do lymph node biopsy today sir
Should we need to send LJ medium culture
[20/12, 08:21]: Yes we should also send it for LJ media culture.
Please check with the microbiology team as to the amount of tissue necessary for that
PaJR PHR Moderator: Let's send two blocks of the tissue to NIMs Punja Gutta also @Participant
I will share a pathology Prof's number there and they may even do it as a free of cost academic second opinion service on request
Participant: @Participant share the biopsy sample images
Participant:



PaJR PHR Moderator: @Participant appears that the pathologists are unaware that the CBNAAT is negative?
Participant: I informed them yesterday sir
They also said that as patient is on ATT since so many months CBNAAT might be negative
PaJR PHR Moderator: Why should it be if it's MDR? Also as long as the bacillus is present why would it be negative? Although now we know the bacillus was actually not present
26/12/24


PaJR PHR Moderator: Thanks
Patient Advocate:

PaJR PHR Moderator: @Participant how's he? No updates for quite some time
Participant: He had no fever 2 days back sir
PaJR PHR Moderator: Was he much better last two weeks after discharge?
Participant: Yes sir
He is getting fever once in 15 days sir
PaJR PHR Moderator: Any update on his lymph node excision and current pel ebstein chart?
Participant: He got admitted under general surgery sir
They r planning to do biopsy tomorrow sir
Participant: Excision done sir


Participant: No sir
PaJR PHR Moderator: Can we share it?

Participant: Histiocytes

11/01/25
Participant:

PaJR PHR Moderator:

12/01/25
Participant:


PaJR PHR Moderator: Is this from MNJ?
PaJR PHR Moderator: 👆Is his IP number here @Participant ? Will need to remember to ask Participant to share his EMR summary tomorrow so that @Narmeen Shah can add the current update in the case report
Participant: No sir
Local lab report
PaJR PHR Moderator: @Narmeen Shah this was the last EMR summary obtained from Participant:
Age/Gender : 57 Years/Male
Discharge Type: Relieved
Admission Date: 03/01/2025 03:53 PM
Date of Operation
Excision BIOPSY DONE ON 7/01/25
Diagnosis
PANCYTOPENIA SECONDARY TO ? HODGKINS LYMPHOMA S/P EXICISION BIOPSY
K/C/O T2 DM SINCE 4 MONTHS
Case History and Clinical Findings
CHEIF COMPLAINTS: K/C/O Cervical LYMADENOPATHY SINCE 9 MONTHS HOPI:
THE PAITENT WAS APPARENTLY ASYMPTOMATIC 9 MONTHS LATER DEVELOPED SWELLINGS ON LEFT SIDE OF THE NECK, WHICH WAS INSIDIOUS ON ONSET. GRADUALLY PROGRESSIVE TO ATTAIN THE CURRENT SIZE.
TRUCUT BIOPSY WAS DONE AND SHOWED LYMPOPROLIFERATICE DISORDER AND OUTSIDE BIOPSY SHOWED ? REACTIVE LYMPADENITIS. AND ADVICED EXCISION BIOPSY H/O FEVER TWICE A MONTH FROM MAY TO OCTOBER AND EVERY 15 DAYS FOR 5 DAYS
SINCE LAST 2 MONTHS
NO H/O COLD,COUGH, NAUSEA, VOMITING, TRAUMA, CONSTIPATION AND LOOSE STOOLS PAST HISTORY:
K/C/O PANCYTOPENIA SECONDARY TO UNKNOWN CONDITIONS. PT WAS ON ATT FOR 5 MONTHS DUE TO H/O TB
K/C/O DM ON TAB METFORMIN 500MG SINCE 4 YEARS GENERAL EXAMINATION:
PT IS C/C/C
NO PALLOR, CLUBBING, ICTERUS, CYANOSIS, EDEMA LYMPHADENOPATHY IS PRESENT - CERVICAL
TEMP- AFEBRILE BP: 130/80MMHG PR: 89BPM
RR: 19CPM SPO2: 99 @ RA
CVS: S1 S2 HEARD, NO MURMURS RS: BAE+
ABDOMEN: SOFT, NT
SURGICAL ONCOLOGY REFERRAL DONE ON 18/12/24
ADVICE USG GUIDED TRUCUT BIOPSY PF LEFT CERVICAL NODE (LARGEST NODE) COURSE IN THE HOSPITAL - PAITENT STARTED ON ATTFROM MAY 29 2024 AND DISGNOSED AS TB LYMPADENTIS ON BASIS OF FNAC REPORT (GRANULOMATOSIS) SINCE THEN PAITENT HAD FEVER FOR EVERY 15 DAYS AND PANCYTOPENIASINCE 2 MONTHS PAITENT WAS ADVICED TO DISCONTINUE ATT AFTER ADMISSION AS PANCYTOPENIA MIGHT HAVE BEEN INDUCED OR AGGRAVATED BY RIFAMPACIN, BUT HEMOGRAM DIDNOT IMPROVE AFTER STOPPING OF ATT BONE MARROW ASPIRATION AND BIOPSY WAS DONE AND FNAC OF LYMPH WAS DONE AND CBNAAT WAS NEGATIVE, SURGICAL ONCOLOGY REFERRAL WAS TAKEN, TRUCUT BIOPSY WAS ADVICED AND DONE ON 20/12/24 SAMPLE SENT FOR HPE WHICH SHOWED LYMPHOPROLIFERATIVE DISORDER, EXCISION AND BIOPSY WAS DONE ON 7/01/2025
Investigation
HBsAg-RAPID 03-01-2025 06:18:PM Negative
Anti HCV Antibodies - RAPID 03-01-2025 06:18:PM Non ReactiveCOMPLETE BLOOD PICTURE (CBP) 03-01-2025 06:18:PMHAEMOGLOBIN 7.9 gm/dl 17.0-13.0 gm/dlTOTAL COUNT 2000
cells/cumm 10000-4000 cells/cummNEUTROPHILS 66 % 80-40 %LYMPHOCYTES 18 % 40-20
%EOSINOPHILS 01 % 6-1 %MONOCYTES 15 % 10-2 %BASOPHILS 00 % 2-0 %PLATELET
COUNT 40,000SMEAR Pancytopenia
COMPLETE URINE EXAMINATION (CUE) 03-01-2025 06:18:PMCOLOUR Pale yellowAPPEARANCE ClearREACTION AcidicSP.GRAVITY 1.010ALBUMIN traceSUGAR +BILE SALTS NilBILE PIGMENTS NilPUS CELLS 3-4EPITHELIAL CELLS 2-3RED BLOOD CELLS NilCRYSTALS NilCASTS NilAMORPHOUS DEPOSITS AbsentOTHERS NilBLOOD UREA 03-01-
2025 06:18:PM 50 mg/dl 42-12 mg/dl
SERUM CREATININE 03-01-2025 06:18:PM 0.7 mg/dl 1.3-0.9 mg/dlSERUM ELECTROLYTES (Na, K, C l) 03-01-2025 06:18:PMSODIUM 132 mmol/L 145-136 mmol/LPOTASSIUM 4.1 mmol/L 5.1-3.5
mmol/LCHLORIDE 101 mmol/L 98-107 mmol/L
LIVER FUNCTION TEST (LFT) 03-01-2025 06:18:PMTotal Bilurubin 1.33 mg/dl 1-0 mg/dlDirect Bilurubin 0.28 mg/dl 0.2-0.0 mg/dlSGOT(AST) 23 IU/L 35-0 IU/LSGPT(ALT) 18 IU/L 45-0
IU/LALKALINE PHOSPHATASE 639 IU/L 128-53 IU/LTOTAL PROTEINS 6.8 gm/dl 8.3-6.4 gm/dlALBUMIN 3.7 gm/dl 5.2-3.5 gm/dlA/G RATIO 1.19POST LUNCH BLOOD SUGAR 03-01-2025
10:02:PM 241 mg/dl 140-0 mg/dl HEMOGRAM DONE ON 8/01/2025
HB: 6.2 GM/DL, WBC: 2000CELLS/CUMM, PLT- 18,000, PCV: 17.%
HEMOGRAM DONE ON 1/01/2025
HB: 7.0 GM/DL, WBC: 2400CELLS/CUMM, PLT- 22,000, PCV: 20.2%
USG NECK DONE
THYROID GLAND -RT LOBE-12X15X38MM,ISTHMUS-1.5 MM, LT LOBE-9X12X37 MM NORMAL S/E AND VASCULARITY
E/O MULTIPLE TINY SPONGIFORM NODULES NOTED IN BOTH LOBES OF THYROID LARGEST MEASURING 8X6 MM IN RIGHT LOBE
E/O MULTIPLE ENLARGED AND PROMINENT CERVICAL LYMPH NODES NOTED BILATERALY IN LEVELS IB,II,III,IV,V LARGEST M 7MM IN LEVEL IV ON RIGHT SIDE AND 31X 18 MM IN LEVEL IB ON LEFT SIDE WITH INTACT FATTY HILUM AND OVOID SHAPE
FEW OF THE LYMPH NODES ARE WITH LOSS OF FATTY HILUM AND OVOID SHAPE. B/L JUGULAR NODES NORMAL
B/L PAROTID AND SUBMANDIBULAR GLANDS NORMAL
E/O ARTHEROSCLEROTIC CHNGES NOTED IN RIGHT CAROTID ARTERY
E/O 4MM CALCIFIED ATHEROSCLEROTIC PLAQUE NOTED IN LEFT ICA JUST DISTAL TO CAROTID BIFURCATION.
IMPRESSION-
-CERVICAL LYMPHADENOPATHY AS DESCRIBED
-SPONGIFOM NODULES IN THYROID AS DESCRIBED
-ATHEROSCLEROTIC CHANGES IN RIGHT CA AND CALCIFIED ATHEROSCLEROTIC PLAQUE IN LEFT ICA.
FNAC DONE ON MAY 2024 (OUTSIDE):-
FEATURES SUGGESTIVE OF GRANULOMATOUS LYMPHADENITIS POSSIBILITY OF KOCHS ETIOLOGY
FNAC DONE ON NOVEMBER 2024 OTSIDE FEATURES SUGGESTIVE OF ATYPICAL,UNDETERMINED SIGNIFICANCE L3. I/V/O RS LIKE MONONUCLEAR CELLS, ADVICED EXCISION BIOPSY FOR FURTHER EVALUATION OF HPE AND IHC STUDY.
FNAC DONE ON 20/12/24-FEATURES SUGGESTIVE OF GRANULOMATOUS/NECROTISING LYMPHADENITIS.
BONE MARROW ASPIRATION DONE ON 30/11/24 IMPRESSION-MICRONORMOBLASTIC PICTURE.
BONE MARROW BIOPSY DONE ON 30/11/24 SECTION STUDIED FROM BONE MARROW BIOPSY SHOWS BITS OF NORMAL TRABECULAR BONE ALONG WITH BONE MARROW ELEMENTS COMPRISING PREDOMINANTLY LYMPHOCYTES,FEW PLASMA CELLS AND OCCASIONAL FOREIGN BODY TYPE GIANT CELLS.
NO DEFINITE GRANULOMATOUS CHANGES SEEN IN STUDIED SECTIONS.ADVICED CLINICAL CORRELATION.
CBNAAT OF FNAC OF LYMPH NODE DONE ON 17/12/24- NEGATIVE
LYMPH NODE BIOPSY DONE ON 20/12/24 AND SENT FOR HISTOPATHOLOGY EXAMINATION IMPRESSION: HISTOLOGICAL FEATURES SUGGESTIVE OF LYMPHOPROLIFERATIVE DISORDER.
EXCISED SPECIM,EN OF LYMPH NODE BIOPSY REPORT: ON 11/1 25
IMPRESSION- HISTOLOGICAL FEATURES ARE COMPATIBLE WITH CLASSIC HODGKINS LYMPHOMA-NODULAR SCLEROSIS.
Treatment Given(Enter only Generic Name)
1. INJ. TAXIM 1GM IV/BD
2. T. PAN 40MGPO/OD
3. T. METFORMIN 500MG PO/BD
4. T. PCM 650MG PO/QID
5. T.CHYMORAL FORTE PO/TID
6. T. LIMCEE PO/OD
7. T. MVT PO/OD
Advice at Discharge
1. TAB METFORMIN 500MG PO/BD X 15DAYS
2. TAB PCM 650MG PO/QID SOS
3. TAB CHYMORALFORTE PO/TID X15DAYS
4. TAB LIMCEE PO/OD X15DAYS
5. TAB MVT PO/OD X15DAYS
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: ______________. For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY
Discharge Date Date: 11/1/25 Ward: AMC Unit:I
PaJR PHR Moderator: Any update?
Partipant: They got admitted in MNJ hospital sir
They transfused prbc and rdp
They r planning to do bone marrow biopsy and pet ct sir
His bilirubin is also increased sir
Patient condition worsened and they shifted him to icu and treating symptamatically sir
PaJR PHR Moderator: Thanks
This will be updated here: https://narmeenshah.blogspot.com/2024/12/57m-tb-cervical-lymphadenopathy.html too @Narmeen Shah
PaJR PHR Moderator: Update from our MRD staff who happens to know the patient:
After getting admitted for one week in the referral cancer hospital, patient's condition steadily deteriorated and he died this Sunday after getting admitted there previous Sunday
Comments
Post a Comment